James Roguski, Dustin Bryce, Lady Xylie, “Pact for the Future”, New Paradigms w/Sargis Sangari EP209
Have a laugh
The Medical Mafia in Action - Offering Isotropic Humanicide Services Worldwide
ABIM = Association of Barbarians for Inquisition in Medicine
ACIP = Assisted Crimes by Immunization from Pandemonium
ACOG = American Consortium of Obstructionists in Gynecopathy
ACOOG = American Consortium of Obstructionists and Obscurantists in Gynecopathy
AHA = Assisted Humanicide Association
AMA = American Murder Association
CDC = Center for Death and Corruption
DIC = Drugs Industrial Complex
DHS = Defense for Humanicide Services
FDA = Fraud and Death Association (Approves Harmaceuticals)
HHS = Holistic Humanicide Services
MD = Mad Doctors
NIAID = Novel Inquisition for Allergic and Infectious Dogmas
NIH = Nihilism In Healthcare
NSFW = Not Safe For Work
USDA = US Department of Absurdity
WEF = World Enslavement Forum (https://files.catbox.moe/r074u2.jpg)
WHO = World Homicide Organization
© 2021 Dr. Red Pill
Copy and paste this to gov. slaves Produced by James Roguski. He is on it
Notice and Statement of Facts:
A collection of excerpts from
court decisions,
government documents,
and articles that have been published
in peer-reviewed medical journals
providing evidence that
the Polymerase Chain Reaction (PCR)
is NOT a valid diagnostic test.
James Roguski
PCR Fraud.com
August 7, 2024
Notice of Facts
You are hereby notified that the facts included in this document clearly show that the use of the RT-PCR
process as a diagnostic “test” is a fraudulent act.
You are also hereby notified that any attempt on your part to coerce, intimidate, mandate, force or
obligate me in any way to undergo such testing will be viewed as an attempt on your part to engage in an
act of fraud and a potential violation of my bodily autonomy and my right of informed dissent to reject
any and all tests and treatments.
Before you continue to attempt to require anyone to undergo RT-PCR “testing” you must be aware that
every man, woman and child always has the unalienable right to REFUSE to undergo any form of health
related treatment, including (and especially) inaccurate and inappropriate procedures that fail to provide
accurate and verifiable diagnoses.
Simply stated, the RT-PCR “test” does not “work,” because RT-PCR is actually a laboratory
manufacturing process that was never designed to be used as a test to diagnose disease. This evidence
includes court decisions from Portugal, Germany and Canada, official government documents and
numerous peer-reviewed articles that have been published in various medical journals.
• The RT-PCR process does not (and cannot) detect viable, infectious viruses.
• The RT-PCR process does not (and cannot) diagnose disease, contagiousness or infectivity.
• The RT-PCR process does not (and cannot) determine whether any specific pathogen is the actual
cause of a disease or any collection of symptoms.
• The RT-PCR process can and does result in false positive results.
Failure to acknowledge the frequency of false positive test results and the subsequent misguided decisions
based on these fraudulent results have led to a plethora of unjustified consequences:
1. Unnecessary contact tracing and fraudulent “testing” has led to the wrongful isolation and
quarantine of men, women and children.
2. Social distancing, mask mandates and loneliness have had negative consequences on human
relations.
3. People have received inaccurate diagnoses and inappropriate medical treatment.
4. Serious diagnoses were wrongly given to terrorized people who were actually in good health.
5. Unprecedented financial, mental, emotional and psychological stress has been inflicted upon
millions of people.
6. Delays in surgical or other procedures and prolonged hospital stays have been experienced.
7. Many employees and small business owners have lost their means of earning a living.
8. Education, travel, dining, leisure and other social activities were curtailed.
9. Clinical trials based on RT-PCR “testing” are meaningless.
10. Epidemiological statistics have been falsified, leading to exaggerated prevalence, hospitalization,
and death rates.
You have 30 days to provide a point by point rebuttal of the following information. Unless and until such
a point by point rebuttal has been provided, it shall stand as accepted fact that the use of the RT-PCR
process as a diagnostic “test” to determine “cases” of disease is a fraudulent use of the technology and
that such testing should never be required of any man, woman, child or of their animals or property.
Statement of Facts:
1. On November 11, 2020, the Court of Appeal of Lisbon (Portugal) ruled that the RT-PCR process
shows itself to be unable to determine beyond reasonable doubt that such positivity corresponds,
in fact, to the infection of a person by the SARS-CoV-2 virus.
2. On April 8, 2021, the Weimar (Germany) Family Court ruled that, effective immediately, two
Weimar schools are prohibited from requiring students to wear mouth-to-nose coverings of any
kind (especially qualified masks such as FFP2 masks), impose minimum AHA distances on them,
and/or participate in SARS-CoV-2 rapid testing.
3. On June 26, 2024, the Ontario (Canada) Court of Justice ruled that people were not obligated to
submit to invasive “testing” such as the nasopharyngeal swab used to collect samples for the RT-
PCR process.
4. The World Health Organization has defined a COVID-19 “case” as a positive PCR test. The
reliance on the RT-PCR process as the sole requirement to determine a COVID-19 “case” without
a differential diagnosis based on clinical observations was essentially unheard of prior to 2020.
5. The RT-PCR process defined in the original “test” (Corman-Drosten) was NOT based upon an
isolated virus. It was based upon a genetic sequence that was compiled in a computer (in silico).
6. The RT-PCR process is NOT a test that can diagnose illness or contagiousness. Its was never
intended to be a diagnostic tool. The PCR process merely creates copies of genetic material found
in a sample. The detection of certain molecules via the RT-PCR process does NOT provide
evidence of disease or contagiousness. The presence of nucleic acids alone should not be used to
infer disease, infection, viral shedding or potential contagiousness.
7. By design, the initial steps in the RT-PCR process destroy the source material so that the RT-PCR
process CANNOT possibly measure intact viruses. A so-called “positive” result does not even
ensure the presence of individual virions.
8. The potential for false positives from use of the RT-PCR process is enormous. Even if the
specificity of a “test” is 99%, if the prevalence of infection in the community is 1/100, then the
“test” will return a false positive result 50% of the time.
9. There is ample evidence that any claims of a “positive” result obtained by running the RT-PCR
process through more than 24 cycles are actually false positives.
10. There is no proof that the nucleic acid sequences that are utilized in any of the various RT-PCR
“tests” identify the presence of a viable pathogen that causes COVID-19. An unknown number of
other pathogens that are NOT being tested for may also be present. Even if the RT-PCR process
identifies the existence of genetic remnants of SARS-CoV-2, it does not rule out the possibility
that something else may be the actual cause of disease.
PCR Fraud.com
1. On November 11, 2020, the Court of Appeal of Lisbon (Portugal) ruled that the RT-PCR process
shows itself to be unable to determine beyond reasonable doubt that such positivity corresponds, in
fact, to the infection of a person by the SARS-CoV-2 virus.
Court of Appeal of Lisbon
The Lisbon Court of Appeal upheld a lower court's decision in support of the writ of habeas corpus that
had been filed by the four German travelers and ruled that the Azores Regional Health Authority had
violated both Portuguese and international law by confining the four German travelers to a hotel. The
judges ruled that only a doctor can “diagnose” someone with a disease, and they were critical of the fact
that the four German travelers were apparently never assessed by a medical doctor.
II. The request made would also be manifestly unfounded because:
A. Prescription and diagnosis are medical acts, the sole responsibility of a doctor, registered with the
Medical Association. Thus, the prescription of auxiliary diagnostic methods (as is the case with viral
infection detection tests), as well as the diagnosis of the existence of a disease, in relation to any and all
people, is a matter that cannot be carried out by Law , Resolution, Decree, Regulation or any other
normative means , as these are acts that our legal system reserves to the exclusive competence of a doctor,
given that he, when advising his patient, must always try to obtain his informed consent.
B. In the case at hand, there is no indication or proof that such a diagnosis was actually carried out by a
professional qualified under the terms of the Law and who had acted in accordance with good medical
practice. In fact, what follows from the facts as established is that none of the applicants was even seen by
a doctor, which is frankly inexplicable, given the alleged severity of the infection.
C. The only element that appears in the proven facts, in this regard, is the carrying out of RT-PCR tests,
one of which showed a positive result in relation to one of the applicants.
D. In view of the current scientific evidence, this test alone proves to be incapable of determining, without
a reasonable margin of doubt, that such positivity corresponds, in fact, to a person's infection with the
SARS-CoV-2 virus, for several reasons, of which we highlight two:
Because this reliability depends on the number of cycles that make up the test;
Because this reliability depends on the amount of viral load present.
III . Any diagnosis or any act of health surveillance... carried out without prior medical observation of the
patients and without the intervention of a doctor registered with the OM (who would carry out the
assessment of their signs and symptoms, as well as examinations that he considered appropriate to his
condition), violates Regulation no. 698/2019, of 5.9, as well as the provisions of article 97 of the Statute
of the Medical Association, being liable to constitute the crime of functions, e.g. and p. by article 358
al.b), of the C.Penal.
IV. Any person or entity that issues an order, the content of which leads to the deprivation of physical,
ambulatory, or other people's freedom (whatever nomenclature this order assumes: confinement,
isolation, quarantine, prophylactic protection, health surveillance, etc.), which does not comply with the
legal provisions, namely the provisions of article 27 of the CRP , you will be carrying out an illegal
detention.
https://www-dgsi-
pt.translate.goog/jtrl.nsf/33182fc732316039802565fa00497eec/79d6ba338dcbe5e28025861f003e7b30?
_x_tr_sl=pt&_x_tr_tl=en&_x_tr_hl=en-US
2. On April 8, 2021, the Weimar (Germany) Family Court ruled that, effective immediately, two
Weimar schools are prohibited from requiring students to wear mouth-to-nose coverings of any
kind (especially qualified masks such as FFP2 masks), impose minimum AHA distances on them,
and/or participate in SARS-CoV-2 rapid testing.
Weimar Family Court in the federal state of Thuringia
The unsuitability of PCR tests and rapid tests for measuring the incidence of infection.
Regarding the PCR test, the court writes: “Already the expert Prof. Dr. med. Kappstein points out in her
expert opinion that only genetic material can be detected with the PCR test used, but not whether the
RNA originates from viruses capable of infection and thus capable of replication (= reproduction).
Also the expert Prof. Dr. rer. biol. hum. Kämmerer also confirms in her expert opinion on molecular
biology that a PCR test – even if it is carried out correctly – cannot provide any information on whether a
person is infected with an active pathogen or not.
This is because the test cannot distinguish between “dead” matter*, e.g. a completely harmless genome
fragment as a remnant of the body’s own immune system’s fight against a cold or flu (such genome
fragments can still be found many months after the immune system has “dealt with” the problem) and
“living” matter, i.e. a “fresh” virus capable of reproducing.
So, even if everything is done “correctly” when performing the PCR including all preparatory steps (PCR
design and establishment, sample collection, preparation and PCR performance), and the test is positive,
i.e.: detects a genome sequence which may also exist in one or even the specific “Corona” virus (SARS-
CoV-2), this does not mean under any circumstances that the person who was tested positive is infected
with a replicating SARS-CoV-2 and consequently infectious = dangerous for other persons.
Rather, for the determination of an active infection with SARS-CoV-2, further, and specifically diagnostic
methods such as the isolation of replicable viruses must be used.
The expert points out that, according to unanimous scientific opinion, all “positive” results that are only
detected after a cycle of 35 have no scientific (i.e.: no evidence-based) basis. In the ct range 26-35, the
test can only be considered positive if matched with viral culture. In contrast, the RT-qPCR test for the
detection of SARS-CoV-2, which was propagated worldwide with the help of the WHO, was (and
following it all other tests based on it as a blueprint) set to 45 cycles without defining a ct value for
“positive”.
Finally, the reviewer points out that the low specificity of the tests causes a high rate of false positives,
which result in unnecessary personnel (quarantine) and societal (e.g., schools closed, “outbreak
notifications”) consequences until they turn out to be false alarms. The error effect, i.e., a high number of
false positives, is particularly strong in tests on symptomless individuals.
It remains to be stated that the PCR test used, as well as the antigen rapid tests, as proven by the expert
opinion, are in principle not suitable for the detection of an infection with the virus SARS-CoV-2.
In addition, the described and other sources of error listed in the expert opinion with serious effects, so
that an adequate determination of the infection with SARS-CoV-2 in Thuringia (and nationwide) is not
rudimentarily available.
https://web.archive.org/web/20210411173241/https://jdfor2024.com/2021/04/reasonable-fact-based-
verdict-from-weimar-germany-no-masks-no-distance-no-more-tests-for-students/
3. On June 26, 2024, the Ontario (Canada) Court of Justice ruled that people were not obligated to
submit to invasive “testing” such as the nasopharyngeal swab used to collect samples for the RT-
PCR process.
Ontario Court of Justice
Ms. Fernando took an airplane flight to her home in Mississauga, arriving at Pearson Airport on April 9th,
2022. She was apparently vaccinated, but she refused the COVID test, which was randomly selected to be
performed on her. In particular, she was sked... to undergo a nasal swab COVID-19 test, and she refused.
Ms. Fernando was convicted at trial of failing to comply with an order under Section 58 of the Quarantine
Act (the “Act”) and fined $5,000 with additional charges, taking it to a fine of $6,255. She appeals now to
this Court.
The argument, simply put, is that the Act did not authorize a screening officer to use a screening test
which involved the entry into the traveller's body of an instrument or other foreign body. The screening
test that Mr. Roxas proposed involved the insertion of a nasal swab into Ms. Fernando's nasal cavity,
contrary to Section 14 of the Quarantine Act.
The relevant provisions are as follows, quoting Section 14 of the Quaranting Act: Screening Technology
14(1) Any qualified person authorized by the Minister may, to determine whether a traveller has a
communicable disease or symptoms of one, use any screening technology authorized by the Minister that
does not involve the entry into the traveller's body of any instrument or other foreign body.
The prosecution raised the point that perhaps the insertion into the nasal cavity did not involve the entry
into the body. I disagree. The insertion of a nasal swab into the nasal cavity is most definitely an insertion
into the body.
I do decide that the nasal swab test, which the screening officer in this case required or demanded Ms.
Fernando submit to, was an unlawful requirement or demand. Ms. Fernando's refusal to comply with the
requirement or demand was lawful on her part. Because the requirement or demand made of her by the
screening officer was not lawful, Ms. Fernando should not have been found guilty by the Justice of the
Peace.
I am reversing the Justice of the Peace's decision and entering a finding of not guilty.
https://canlii.ca/t/k5q3t
4. The World Health Organization has defined a COVID-19 “case” as a positive PCR test. The
reliance on the RT-PCR process as the sole requirement to determine a COVID-19 “case” without a
differential diagnosis based on clinical observations was essentially unheard of prior to 2020.
March 20, 2020:
Confirmed case: A person with laboratory confirmation of COVID-19 infection, irrespective of clinical
signs and symptoms.
https://web.archive.org/web/20200624130127/https://www.who.int/publications-detail-redirect/global-
surveillance-for-covid-19-caused-by-human-infection-with-covid-19-virus-interim-guidance
https://web.archive.org/web/20200624130127/https://apps.who.int/iris/rest/bitstreams/1272502/retrieve
December 16, 2020:
https://web.archive.org/web/20201223174118/https://www.who.int/publications/i/item/WHO-2019-
nCoV-Surveillance_Case_Definition-2020.2
https://web.archive.org/web/20201223103839/https://apps.who.int/iris/rest/bitstreams/1322790/retrieve
July 22, 2022 to present day:
https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2022.1
https://iris.who.int/bitstream/handle/10665/360579/WHO-2019-nCoV-Surveillance-Case-Definition-
2022.1-eng.pdf
International Journal of Vaccine Theory, Practice, and Research
For the first time in medical history, a laboratory assay (RT-PCR) was used as the sole criterion to
diagnose a disease (COVID-19) and to define infectivity of a virus (SARS-CoV-2) without rating clinical
symptoms and proof of replication-competent virus to justify implementing population-wide, untested
interventions.
Unnecessary quarantine of healthy individuals, as well as lockdowns and atrocious collateral damage on
societies and economies worldwide due to a high number of false-positive “PCR-cases.” Otherwise,
infectious symptomatic individuals were given a false sense of security by false-negative test results,
which could lead to COVID-19 clusters. Both our results and literature data confirm that validation of any
PCR-based diagnostic test by sequencing is mandatory on a regular basis. To prevent future misconduct,
science needs a reality check and must re-initiate the scientific dialogue and liberate itself from political
influence and dogma.
https://ijvtpr.com/index.php/IJVTPR/article/view/71
International Journal of Vaccine Theory, Practice, and Research
PCR testing has been erroneously chosen as the gold standard for diagnosing COVID-19 infection and
disease, even if it has never been validated, nor standardized. The symptoms of COVID-19 disease cannot
be specified, because they can be anything, everything, and nothing at all according to the authorities.
They range from clinically observable symptoms likely to lead to death to no symptoms at all — from
near death to complete health. All the foregoing shows the entire scope of COVID-19 diagnostic science
is flawed.
https://ijvtpr.com/index.php/IJVTPR/article/view/81/216
5. The RT-PCR process defined in the original “test” (Corman-Drosten) was NOT based upon an
isolated virus. It was based upon a genetic sequence that was compiled in a computer (in silico).
The Corman-Drosten paper contains the following specific errors:
1. There exists no specified reason to use these extremely high concentrations of primers in this
protocol. The described concentrations lead to increased nonspecific bindings and PCR product
amplifications, making the test unsuitable as a specific diagnostic tool to identify the SARS-CoV-
2 virus.
2. Six unspecified wobbly positions will introduce an enormous variability in the real world
laboratory implementations of this test; the confusing nonspecific description in the Corman-
Drosten paper is not suitable as a Standard Operational Protocol making the test unsuitable as a
specific diagnostic tool to identify the SARS-CoV-2 virus.
3. The test cannot discriminate between the whole virus and viral fragments. Therefore, the test
cannot be used as a diagnostic for intact (infectious) viruses, making the test unsuitable as a
specific diagnostic tool to identify the SARS-CoV-2 virus and make inferences about the
presence of an infection.
4. A difference of 10° C with respect to the annealing temperature Tm for primer pair1
(RdRp_SARSr_F and RdRp_SARSr_R) also makes the test unsuitable as a specific diagnostic
tool to identify the SARS-CoV-2 virus.
5. A severe error is the omission of a Ct value at which a sample is considered positive and
negative. This Ct value is also not found in follow-up submissions making the test unsuitable as a
specific diagnostic tool to identify the SARS-CoV-2 virus.
6. The PCR products have not been validated at the molecular level. This fact makes the protocol
useless as a specific diagnostic tool to identify the SARS-CoV-2 virus.
7. The PCR test contains neither a unique positive control to evaluate its specificity for SARS-CoV-
2 nor a negative control to exclude the presence of other coronaviruses, making the test unsuitable
as a specific diagnostic tool to identify the SARS-CoV-2 virus.
8. The test design in the Corman-Drosten paper is so vague and flawed that one can go in dozens of
different directions; nothing is standardized and there is no SOP. This highly questions the
scientific validity of the test and makes it unsuitable as a specific diagnostic tool to identify the
SARS-CoV-2 virus.
9. Most likely, the Corman-Drosten paper was not peer-reviewed making the test unsuitable as a
specific diagnostic tool to identify the SARS-CoV-2 virus.
10. We find severe conflicts of interest for at least four authors, in addition to the fact that two of the
authors of the Corman-Drosten paper (Christian Drosten and Chantal Reusken) are members of
the editorial board of Eurosurveillance. A conflict of interest was added on July 29 2020 (Olfert
Landt is CEO of TIB-Molbiol; Marco Kaiser is senior researcher at GenExpress and serves as
scientific advisor for TIB-Molbiol), that was not declared in the original version (and still is
missing in the PubMed version); TIB-Molbiol is the company which was “the first” to produce
PCR kits (Light Mix) based on the protocol published in the Corman-Drosten manuscript, and
according to their own words, they distributed these PCR-test kits before the publication was
even submitted [20]; further, Victor Corman & Christian Drosten failed to mention their second
affiliation: the commercial test laboratory “Labor Berlin”. Both are responsible for the virus
diagnostics there [21] and the company operates in the realm of real time PCR-testing.
In light of our re-examination of the test protocol to identify SARS-CoV-2 described in the Corman-
Drosten paper we have identified concerning errors and inherent fallacies which render the SARS-CoV-2
PCR test useless.
https://web.archive.org/web/20220923083309/https://cormandrostenreview.com/report/
6. The RT-PCR process is NOT a test that can diagnose illness or contagiousness. Its was never
intended to be a diagnostic tool. The PCR process merely creates copies of genetic material found in
a sample. The detection of certain molecules via the RT-PCR process does NOT provide evidence of
disease or contagiousness. The presence of nucleic acids alone should not be used to infer disease,
infection, viral shedding or potential contagiousness.
Canada
A person is deemed infectious if they shed virus particles that are intact and able to go on to infect others.
PCR tests cannot distinguish viral genomic material coming from intact viral particles in persons who are
infectious or viral particle fragments that are present in individuals who have recovered.
We do not know how much virus is actually required to cause an infection in someone and there are other
important factors that may influence infectiousness, including the health of the person exposed and the
type of exposure that has happened.
https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-
documents/polymerase-chain-reaction-cycle-threshold-values-testing.html
The CDC
Detection of viral nucleic acid is not equivalent to isolating a virus.
https://wwwnc.cdc.gov/eid/article/7/4/01-7431_article
A positive result indicates detection of influenza viral RNA or nucleic acids in the respiratory specimen
tested, confirming influenza virus infection, but does not necessarily mean infectious virus is present or
that the patient is contagious.
https://www.cdc.gov/flu/professionals/diagnosis/molecular-assays.htm
New Zealand
A positive test cannot tell us:
if the person is currently infectious
how ill the person is likely to become.
https://web.archive.org/web/20210122000504/https://www.health.govt.nz/our-work/diseases-and-
conditions/covid-19-novel-coronavirus/covid-19-health-advice-public/assessment-and-testing-covid-
19/covid-19-test-results-and-their-accuracy
Singapore
It is important to note that viral RNA detection by PCR does not equate to infectiousness or viable virus.
https://www.ncid.sg/Documents/Period%20of%20Infectivity%20Position%20Statementv2.pdf
Sweden
Comparisons of results with PCR detection of viruses and virus culture shows that PCR cannot be used to
determine whether an individual remains contagious or not because PCR also detects RNA from non-
infectious viruses. Sampling by PCR to determine infectiousness should therefore be avoided.
https://kommun.falkenberg.se/images/sv/files/vagledning-om-smittsamhetsbedomning-vid-covid-
19%C3%85H.pdf (pages 6-7)
United Kingdom
A single Ct value in the absence of clinical context cannot be relied upon for decision making about a
person’s infectivity.
RT-PCR detects presence of viral genetic material in a sample but is not able to distinguish whether
infectious virus is present.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/926410
/Understanding_Cycle_Threshold__Ct__in_SARS-CoV-2_RT-PCR_.pdf
Nature Reviews Microbiology
Although detection of viral RNA in respiratory specimens by RT-PCR is highly sensitive and specific, it
does not distinguish between replication-competent virus and residual RNA.
RT-PCR cannot directly determine infectiousness owing to its inability to differentiate between
replication-competent (infectious) virus and residual (non-infectious) viral RNA.
Unfortunately, no point-of-care diagnostic test currently exists to determine infectious SARS-CoV-2 in a
patient sample.
To date, no diagnostic tests exist that reliably determine the presence of infectious virus.
https://www.nature.com/articles/s41579-022-00822-w
The Lancet
Although the use of sensitive PCR methods offers value from a diagnostic viewpoint, caution is required
when applying such data to assess the duration of viral shedding and infection potential because PCR
does not distinguish between infectious virus and non-infectious nucleic acid.
The presence of nucleic acid alone cannot be used to define viral shedding or infection potential.
For many viral diseases (SARS-CoV, Middle East respiratory syndrome coronavirus, influenza virus,
Ebola virus, and Zika virus) it is well known that viral RNA can be detected long after the disappearance
of infectious virus.
The immune system can neutralise viruses by lysing their envelope or aggregating virus particles; these
processes prevent subsequent infection but do not eliminate nucleic acid, which degrades slowly over
time.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30868-0/fulltext
Clinical Infectious Diseases
Complete live viruses are necessary for transmission, not the fragments identified by PCR.
https://academic.oup.com/cid/article/73/11/e3884/6018217
Clinical Infectious Diseases
A positive RT-qPCR result may not necessarily mean the person is still infectious or that he or she still
has any meaningful disease.
The RNA could be from nonviable or killed virus. Live virus is often isolable only during the first week
of symptoms but not after day 8, even with positive RT-qPCR tests.
https://academic.oup.com/cid/article/71/16/2252/5841456
Cleveland Clinic
The test can continue to detect fragments of SARS-CoV-2 virus even after you’ve recovered from
COVID-19 and are no longer contagious. So you may continue to test positive if you've had COVID-19
in the distant past, even though you can’t spread the SARS-CoV-2 virus to others.
https://my.clevelandclinic.org/health/diagnostics/21462-covid-19-and-pcr-testing
7. By design, the initial steps in the RT-PCR process destroy the source material so that the RT-
PCR process CANNOT possibly measure intact viruses. A so-called “positive” result does not even
ensure the presence of individual virions.
Sample preparation excludes the detection of replication- capable viruses.
A PCR test - even if performed correctly - cannot provide any information on whether a person is infected
with an active pathogen or not.
This is technically impossible, because the test procedure includes a complete destruction of the
biological material and separation of nucleic acids from all other material, thus destroying any structure
necessary for biological function like replication and infection.
This is because the test cannot distinguish between "dead" matter*, such as a completely harmless
genome fragment as a remnant of the body's own immune system's fight against a cold or flu (such
genome fragments can still be found many months after the immune system has "dealt with" the
problem), and "living" matter, i.e. a "fresh", reproducible virus.
A crucial step in this process is the complete denaturation of all biological material and separation of the
main components protein, lipids and nucleic acids in order to finally have the RNA available as a starting
base for RT- qPCR.
The original protocol of Chomszynski and Sacci from 1987 is still a component of almost all protocols for
the purification of biological material for RNA isolation, whether prepared in the laboratory or in
purchased "extraction kits." Components of the original extraction solution are phenol/chloroform and
isoamyl alcohol, and in various modified commercial solutions [are] similarly acting but less toxic
substances.
All have in common that they completely destroy any living or reproducible biological structure.
In the laboratory process of preparing a smear sample, which is mandatory preceeding the RT-qPCR, any
biological material, be it a vital cell, a replicable virus or even just cell debris and gene residues, is
denatured in such a way, that it is no longer possible to say whether the material originates from an intact
or even replication competent organism or from samples that have already been damaged or destroyed.
Due to this extraction and preparation process, a positive RT-qPCR that detects genome fragments cannot
be used to infer the presence of replication-capable viruses in the smear sample.
Thus, even if the PCR, including all preparatory steps (PCR design and establishment, sample collection,
preparation and PCR performance), is carried out "correctly", and the test is positive, i.e.: detects a
genome sequence which may also exist in one or even the specific "Corona" virus (SARS-CoV-2), this
technique can under no circumstances prove that the person who tested positive could be infected with a
replicating SARS-CoV-2 and consequently infectious = dangerous for other persons.
Expert opinion by Prof. Dr. rer. biol. hum. Ulrike Kämmerer
8. The potential for false positives from use of the RT-PCR process is enormous. Even if the
specificity of a “test” is 99%, if the prevalence of infection in the community is 1/100, then the
“test” will return a false positive result 50% of the time.
United Kingdom
What causes false positives?
Cross reactions with other genetic material. Other sources of DNA or RNA may have cross reactive
genetic material that can be amplified by the RT-PCR test. False positives were observed unexpectedly in
norovirus assays in patients with enterocolitis, due to unusually high levels of human DNA in samples.
Contamination during sampling. This may happen if the swab head accidently contacts, or is placed on a
contaminated surface (for example, latex gloves, hospital surface).
Contamination during swab extraction. Viral RNA is extracted from swabs in solution; accidental
aerosolization of liquid can cause cross contamination between samples.
Contamination with PCR amplicon. The PCR amplification process generates millions of copies of the
DNA target (amplicon) that can cause false positives in subsequent PCR reactions. If a testing lab is
accidently contaminated with amplicon it can lead to sporadic false positives.
Contamination of PCR laboratory consumables. Contamination can spread from a post-PCR lab into a
pre-PCR lab by transfer of equipment, chemicals, people or aerosol. Even experienced national labs can
be affected. In early-March 2020, COVID-19 RT-PCR assays produced by the CDC were withdrawn after
many showed false positives due to contaminated reagents.
https://www.gov.uk/government/publications/gos-impact-of-false-positives-and-negatives-3-june-
2020/impact-of-false-positives-and-false-negatives-in-the-uks-covid-19-rt-pcr-testing-programme-3-june-
2020
World Health Organization
WHO reminds [In Vitro Diagnostic Medical Device] IVD users that disease prevalence alters the
predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2).
This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly
infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.
https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
FDA
Positive and negative predictive values are highly dependent on prevalence. False-negative test results are
more likely when prevalence of disease is high. False-positive test results are more likely when
prevalence is moderate to low.
https://www.fda.gov/media/134922/download
FDA
Remember that positive predictive value (PPV) varies with disease prevalence when interpreting results
from diagnostic tests. PPV is the percent of positive test results that are true positives. As disease
prevalence decreases, the percent of test results that are false positives increase.
For example, a test with 98% specificity would have a PPV of just over 80% in a population with 10%
prevalence, meaning 20 out of 100 positive results would be false positives.
The same test would only have a PPV of approximately 30% in a population with 1% prevalence,
meaning 70 out of 100 positive results would be false positives. This means that, in a population with 1%
prevalence, only 30% of individuals with positive test results actually have the disease.
At 0.1% prevalence, the PPV would only be 4%, meaning that 96 out of 100 positive results would be
false positives.
Health care providers should take the local prevalence into consideration when interpreting diagnostic test
results.
https://web.archive.org/web/20201113085851/https://www.fda.gov/medical-devices/letters-health-care-
providers/potential-false-positive-results-antigen-tests-rapid-detection-sars-cov-2-letter-clinical-
laboratory
The Lancet
The widespread use of PCR in clinical settings has been hampered largely by background contamination
from exogenous sources of DNA. In most pathogen-specific assays, the predominant source of
contamination is derived from “carryover” products from earlier PCR reactions, which can be harboured
and transmitted through PCR reagents, tubes, pipettes, and laboratory surfaces. Coupled with the robust
amplification power of PCR, even very minor amounts of carry-over contamination may serve as
substrates for amplification and lead to false-positive results.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7106425/
Journal of Infection
In light of our findings that more than half of individuals with positive PCR test results are unlikely to
have been infectious, RT-PCR test positivity should not be taken as an accurate measure of infectious
SARS-CoV-2 incidence. Our results confirm the findings of others that the routine use of “positive” RT-
PCR test results as the gold standard for assessing and controlling infectiousness fails to reflect the fact
“that 50-75% of the time an individual is PCR positive, they are likely to be post-infectious
There is no international standardization across laboratories, rendering problematic the interpretation of
RT-PCR tests when used as a tool for mass screening.
https://www.journalofinfection.com/article/S0163-4453(21)00265-6/fulltext
The Royal College of Pathologists of Australasia
Timely identification of true false positive SARS-CoV-2 NAT results is important as unrecognised false
positive results can lead to unnecessary quarantining and contact tracing, delays in the recognition and
treatment of the true illness, significant patient anxiety and concern, potential exposure to nosocomial
infection from other patients with confirmed COVID-19, wastage of personal protective equipment, and
inaccurate statistics regarding local prevalence of infection.
https://www.pathologyjournal.rcpa.edu.au/article/S0031-3025(20)30936-3/fulltext
Clinical Medicine
Several potential significant implications for the single-gene low-level false positive results were
recognised. Patients on the transplant waiting list were removed from the list for 2 weeks. Some of the
patients screened pre-operatively had their surgery delayed. Patients screened pre-discharge were kept in
hospital, unnecessarily in many cases.
Implications of false positive results
• unnecessary treatment and investigation
• missing or delayed surgery
• unnecessary isolation and contact tracing with subsequent negative impact on workforce and
resources
• a risk of subsequent increased exposure if the individual changes their behaviour as a result of
believing that they have been infected
• the individual being placed with other inpatients with COVID-19 and consequently exposed to
the virus.
A major risk of a false positive result occurs when the individual is cohorted with other patients suffering
from COVID-19 and is consequently exposed to the virus.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7850182/
Journal of Occupational and Environmental Medicine
The performance of these tests when deployed depends not only on their clinical sensitivities and
specificities, but also the prevalence of SARS-CoV-2 infections in the setting in which the test is being
used. If we consider a test that conforms to the FDA's recommendations for performance in a… screening
setting (95% sensitivity, 98% specificity).
For the screening scenario, 100 of the 10,000 individuals are infected and 9900 are not. The test will
detect 95 of the infected persons and five will be falsely negative. For those who are not infected, 9702
will be correctly diagnosed and 198 will be false positives. The PPV is 95/95 + 198 or 32.4%. In this case,
2/3 of the positive results are false positives. For a prevalence of 0.1%, the PPV drops to 4.5%.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7934325/
9. There is ample evidence that any claims of a “positive” result obtained by running the RT-PCR
process through more than 24 cycles are actually false positives.
World Health Organization
Careful interpretation of weak positive NAAT results is needed, as some of the assays have shown to
produce false signals at high Ct values.
https://iris.who.int/bitstream/handle/10665/334254/WHO-2019-nCoV-laboratory-2020.6-eng.pdf
Canada
A frequent question is whether Ct values can help determine whether an individual is infectious or not. It
is not possible to directly translate a Ct value into degree or duration of infectiousness.
https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-
documents/polymerase-chain-reaction-cycle-threshold-values-testing.html
Clinical Infectious Diseases
At Ct = 35, the value we used to report a positive result for PCR, <3% of cultures are positive.
https://academic.oup.com/cid/article/72/11/e921/5912603
Clinical Infectious Diseases
Many qPCR assays involve a Ct cutoff of 40 to consider the test positive, allowing detection of very few
starting RNA molecules.
However, reporting as a binary positive or negative result removes useful information that could inform
clinical decision making.
Following complete resolution of symptoms, people can have prolonged positive SARS-CoV-2 RT-PCR
test results, potentially for weeks, as Xiao et al report. At these late time points, the Ct value is often very
high, representing the presence of very low copies of viral RNA [5–8]. In these cases, where viral RNA
copies in the sample may be fewer than 100, results are reported to the clinician simply as positive. This
leaves the clinician with little choice but to interpret the results no differently than for a sample from
someone who is floridly positive and where RNA copies routinely reach 100 million or more.
A positive RT-qPCR result may not necessarily mean the person is still infectious or that he or she still
has any meaningful disease. First, the RNA could be from nonviable or killed virus. Live virus is often
isolable only during the first week of symptoms but not after day 8, even with positive RT-qPCR tests [9].
Second, there may need to be a minimum amount of viable virus for onward transmission. For infection
control purposes, the utility of the assay is greatest when identifying people who are floridly positive and
at risk of further transmission. Particularly when testing in the absence of symptoms for COVID-19, we
believe that reporting the Ct value or range could help to better inform clinical decisions.
https://academic.oup.com/cid/article/71/16/2252/5841456
Clinical Infectious Diseases
Above a CT value of 24, the amount of detectable viral genetic material is so low that the positive test
could no longer be interpreted in terms of an active infection.
https://academic.oup.com/cid/article/71/10/2663/5842165
European Journal of Clinical Microbiology & Infectious Diseases
We can deduce that with our system, patients with Ct values equal or above 34 do not excrete infectious
viral particles.
https://link.springer.com/article/10.1007/s10096-020-03913-9
The New England Journal of Medicine
Viral culture was positive only in samples with a cycle-threshold value of 28.4 or less.
https://www.nejm.org/doi/full/10.1056/NEJMc2027040
10. There is no proof that the nucleic acid sequences that are utilized in any of the various RT-PCR
“tests” identify the presence of a viable pathogen that causes COVID-19. An unknown number of
other pathogens that are NOT being tested for may also be present. Even if the RT-PCR process
identifies the existence of genetic remnants of SARS-CoV-2, it does not rule out the possibility that
something else may be the actual cause of disease.
World Health Organization
Co-infections of SARS-CoV-2 with other pathogens have been reported, thus a positive test for another
pathogen does not rule out COVID-19 and vice versa.
https://iris.who.int/bitstream/handle/10665/334254/WHO-2019-nCoV-laboratory-2020.6-eng.pdf
FDA
Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the
causative agent for clinical symptoms. This test cannot rule out diseases caused by other bacterial or viral
pathogens.
https://www.fda.gov/media/134922/download
FDA
Clinical correlation with patient history and other diagnostic information is necessary to determine patient
infection status. Positive results do not rule out bacterial infection or co-infection with other viruses.
https://www.fda.gov/media/137093/download
Eurosurveillance
In total, we have tested to date (as at 19 February 2020) 4,084 respiratory samples by PCR and all the
tests have been negative for SARS-CoV-2.
These tests were carried out on the samples of 32 suspected SARS-CoV-2 cases, 337 people repatriated at
the beginning of February 2020 from China tested twice, 164 patients who died in public hospitals in
Marseille between 2014 and 2019 of whom at least one respiratory sample had been sent to our
laboratory, and they also included 3,214 respiratory samples sent since January 2020 to our laboratory to
search for a viral aetiology.
In striking contrast, we have tested 5,080 respiratory samples for various suspected respiratory viral
infections since 1 January 2020 and identified in 3,380 cases respiratory viruses. In decreasing order of
frequency, they were: influenza A virus (n = 794), influenza B virus (n = 588), rhinovirus (n = 567),
respiratory syncytial virus (n = 361), adenovirus (n = 226), metapneumovirus (n = 192), enterovirus
(n = 171), bocavirus (n = 83), parainfluenza virus (n = 24), and parechovirus (n = 8). Among the diagnosed
viruses, there were also 373 common human coronaviruses (HCoV), including 205 HCoV-HKU1, 94
HCoV-NL63, 46 HCoV-OC43, and 28 HCoV-229E [5].
Thus, it is surprising to see that all the attention focused on a virus whose mortality ultimately appears to
be of the same order of magnitude as that of common coronaviruses or other respiratory viruses such as
influenza or respiratory syncytial virus, while the four common HCoV diagnosed go unnoticed although
their incidence is high.
https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.8.2000171
Clinical Chemistry and Laboratory Medicine
A total of 239 positive targets of pathogens were detected in 161 children. The highest proportion of
pathogens were human respiratory syncytial virus (HRSV) (in 76 patients [31.80%]) and influenza A
virus (in 72 patients [30.13%]). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the
virus that causes COVID-19, was detected in two patients and accounted for 0.84%.
SARS-COV-2, HRSV and human metapneumovirus (HMPV) were found in the bronchoalveolar lavage
fluid of patient 1, and SARS-COV-2, MP and HMPV were found in the bronchoalveolar lavage fluid of
patient 2.
https://www.degruyter.com/document/doi/10.1515/cclm-2020-0434/html
The Lancet [Comment]
In our view, current PCR testing is therefore not the appropriate gold standard for evaluating a SARS-
CoV-2 public health test.
The short window of transmissibility contrasts with a median 22–33 days of PCR positivity (longer with
severe infections and somewhat shorter among asymptomatic individuals). This suggests that 50–75% of
the time an individual is PCR positive, they are likely to be post-infectious.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00425-6/fulltext
International Journal of Vaccine Theory, Practice, and Research
It was revealed that a positive RT-qPCR test still harbors the risk of picking up something other than
SARS-CoV-2 alone. Samples from primary care patients suspicious for SARS-CoV-2, since the patients
presented themselves with clinical symptoms of a respiratory infection, after RT-qPCR, were found to be
positive for other viral and bacterial pathogens and even human genomic DNA (Voogd et al., 2022).
Thus, solely trusting the outcome of a positive RT-qPCR test result risks a wrong diagnosis even with
optimized commercial kits.
All that being said, nevertheless, we believe there was a grossly negligent omission during the COVID-19
pandemic: regular and sufficient negative and positive controls did not exclude the co-presence of
pathogen(s) other than SARS-CoV-2(except in the just-mentioned Killingley experiment) which might be
causing the observed COVID-19 disease symptoms. Additionally, the symptoms used in diagnosis are so
general and common in respiratory diseases that it “... may not be possible to distinguish among the viral
diseases under study judging only by the clinical presentation” (Czubak et al., 2021). Among the disease
agents that cannot be definitively excluded are seasonal flu viruses which have been identified as co-
infective by Wuhan researchers (Yue et al., 2020) in some persons diagnosed withSARS-CoV-2 infection.
Given that there are no “virus-type-specific” therapies that distinguish all the types of respiratory viruses,
molecular diagnostics hardly have anything more than mere academic value. The critical information
guiding the choice of therapies would need to take account of co-infecting bacteria and fungi possibly
accompanying any respiratory viruses and for which a specific therapy could have helped or even saved
the lives of many victims —such as those “COVID-19 patients” who died with non-detected aspergillus
and might have survived on anti-fungal therapy (Evert et al., 2021).
We assert that testing asymptomatic people is useless.
https://ijvtpr.com/index.php/IJVTPR/article/view/82/217Lorem ipsum dolor
Professor Ian Duncan
Head of the UK Office of National Statistics (ONS) ignores data request from 7 Members of Parliament
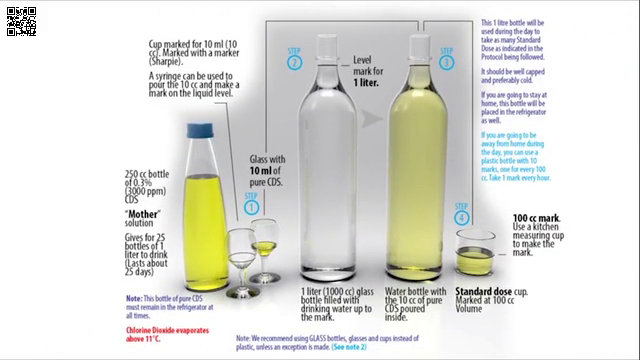
Info on using Chlorine Dioxide
I am VERY concerned that the people involved in this debate are going to avoid the 12 most important FACTS:
1 The FACT that the UK government was one of the nations that illegitimately submitted amendments to the 75th World Health Assembly on May 24, 2022, in violation of Article 55 of the International Health Regulations which require 4 months advance notice. DETAILS
2 The FACT the the WHO has fraudulently presented the 2022 amendments as having been voted upon on May 28, 2022, when no such vote ever happened. DETAILS THEY LITERALLY LIED ABOUT THE VOTE
3 The FACT that the request put forth in the UK Parliament petition was designed to trigger a debate BEFORE the December 1, 2023 deadline to reject the 2022 amendments to the International Health Regulations, but this debate is obviously happening after that deadline has passed. DETAILS
4 The FACT that the Foreign, Commonwealth and Development Office absolutely failed in its duty to submit the 2022 amendments to the UK Parliament for a 21 day review, and their potential rejection, as required by UK law. DETAILS
5 The FACT that the Working Group for amendments to the International Health Regulations is openly conspiring to violate Article 55 of the International Health Regulations by failing to submit a final package of targeted amendments to the WHO at least 4 months in advance of the 77th World Health Assembly (before January 27, 2024). DETAILS
6 The FACT that the Working Group for amendments to the International Health Regulations are overstepping their authority under Article 21 of the WHO Constitution. DETAILS
7 The FACT that the WHO is already building and planning to implement the Global Digital Health Certification Network even though the negotiations to amend the International Health Regulations to include such an expansion of control have not yet come to an official agreement. DETAILS
8 The FACT that there has been no official opportunity whatsoever for the public to submit comments to either the WHO or the UK Government regarding the 2022 amendments or the proposed 2024 amendments to the International Health Regulations.
9 The FACT that approval by the UK Parliament is NOT NEEDED AND NEITHER THE APPROVAL NOR THE CONSENT OF PARLIAMENT WILL BE SOUGHT in order for the amendments to be accepted by the executive branch of the UK Government. No such approval was sough or given for the 1969 International Health Regulations, the 2005 amendments or the 2022 amendments.
10 The FACT that the negotiations have been conducted in secret for over one year and the latest version of the proposed amendments has not been made available to any Member of Parliament (or any legislator anywhere on earth).
11 The FACT that Parliamentary petitions to discuss the 2022 amendments were signed by thousands of people in Australia (55,697), Canada (18,973) and New Zealand (26,120) and were completely ignored by their governments and NOT A SINGLE LEGISLATIVE BODY ON EARTH EVER DISCUSSED OR VOTED TO APPROVE THE FRAUDULENTLY ADOPTED 2022 AMENDMENTS.
12 The FACT that for 76+ years, the World Health Assembly has failed to EVER adopt regulations for any of the issues in Article 21, sections b, c, d, and e listed below. Their complete and total failure to set standards in the past, and their complete and total failure to even consider any amendments regarding these issues during the current negotiations is absolutely UNACCEPTABLE.
WHO CONSTITUTION
ARTICLE 21
(b) nomenclatures with respect to diseases, causes of death and public health practices;
(c) standards with respect to diagnostic procedures for international use;
(d) standards with respect to the safety, purity and potency of biological, pharmaceutical and similar products moving in international commerce;
(e) advertising and labelling of biological, pharmaceutical and similar products moving in international commerce.
World Health Organization
Tedros Adhanom Ghebreyesus
Director-General
Avenue Appia 20
1211 Geneva
Switzerland
Notice to agent is notice to principal. Notice to principal is notice to agent.
Dear Director-General Ghebreyesus,
This letter is to inform you of my rejection of the amendments to the International Health Regulations that were adopted by the 75th World Health Assembly on May 27, 2022. Articles 59 and 61 of the International Health Regulations clearly specify that amendments may be rejected within 18 months of formal notification of their adoption.
I hereby REJECT these amendments and challenge the legitimacy of their purported adoption due to the fact that they were submitted in violation of Article 55 of the International Health Regulations.
These amendments were first submitted to the World Health Assembly on May 24, 2022 by Australia, Bosnia and Herzegovina, Colombia, the European Union and its Member States, Japan, Monaco, the Republic of Korea, the United Kingdom of Great Britain and Northern Ireland and the United States of America.
https://apps.who.int/gb/ebwha/pdf_files/WHA75/A75_ACONF7-en.pdf
The submission of these proposed amendments during the 75th World Health Assembly was in clear violation of Article 55, Section 2 of the International Health Regulations which states:
“The text of any proposed amendment shall be communicated to all States Parties by the Director-General at least four months before the Health Assembly at which it is proposed for consideration.”
The International Health Regulations:
https://iris.who.int/bitstream/handle/10665/246107/9789241580496-eng.pdf
The version of the amendments to the IHR that were adopted on May 27, 2022:
https://apps.who.int/gb/ebwha/pdf_files/WHA75/A75_ACONF7Rev1-en.pdf
Video recording of the amendments being adopted:
https://www.youtube.com/watch?v=M393lvg1650&t=466s
The amended Articles to the IHR:
https://apps.who.int/gb/ebwha/pdf_files/WHA75/A75_R12-en.pdf
The amendments were illegitimately submitted and must be treated by all states parties as being null and void.
Sincerely,
UK resident
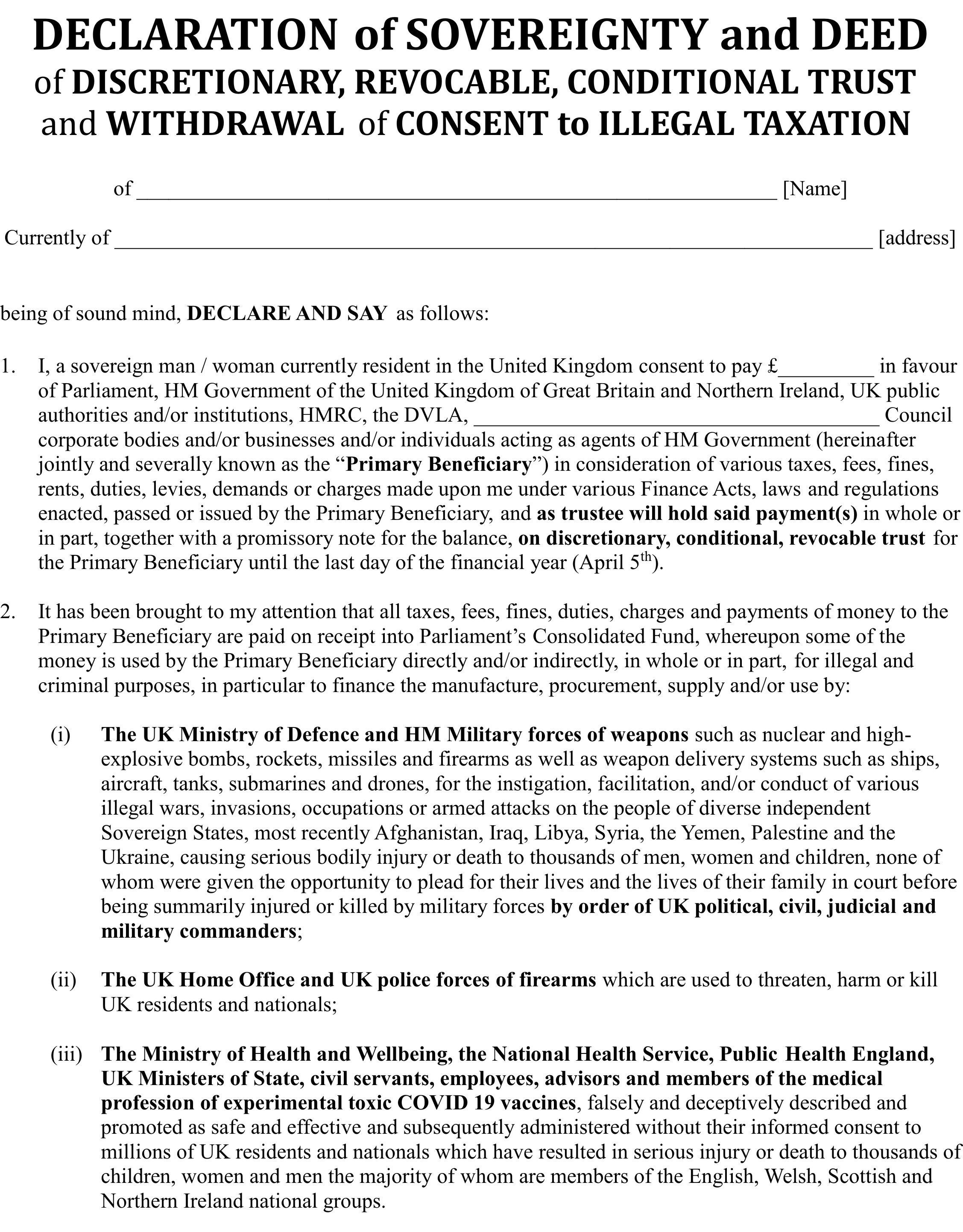
Gallery
Serious Do it NOW. Download copy print distribute

You could print and distribute this below. It is clear when opened with a right click view or save. It includes a contact link for UN so you can send a message, maybe the peoples declaration. Just saves some time figuring it out. Only have a few days before the UN WHO wrap up the program and continue with agenda 21-30 of fake pandemics (bioweapons) and Global boiling (their words) fraud,
This is a jpeg image of an A4 flyer.
Links: